


Understanding The Upper Trapezius
Doctor of Chiropractic, Dr. Alex Jimenez explores the relevant anatomy and function of the UT, the role it has in musculoskeletal dysfunction and management ideas in the form of strengthening and loosening.
The upper trapezius (UT) is a major muscle that affects movement and stability of both the scapula and cervical spine. The coordination and interplay between the UT and other scapula muscles such as the lower and middle trapezius, serratus anterior, rhomboids, levator scapulae and pectoralis minor, have a large bearing on how the scapula moves and how stable it can become to allow proper gleno-humeral motion. With this in mind, dysfunction in the UT, either as weakness or hypertonicity, has been implicated in a host of shoulder pathologies and cervical spine syndromes.
Anatomy &Â Biomechanics
The gross anatomy and function of the UT is comprehensively discussed in a landmark study from the 1990’s(1). Johnson and Bogduk (1994) dissected the individual fascicular anatomy of the UT from the superior nuchal line near the occiput, all the way down to the C7 vertebrae, and also the thoracic portion of the
UT. What they found was that the UT was a multipennate muscle that had no osseous attachments between the occiput to the C7 spinous process. Instead the UT originated from the fascial structure known as the ‘ligamentum nuchae’.
The upper cervical fibres from C1 to C6 passed in a downward direction, and traversed to insert into the clavicle. Fibres from C7 and T1 passed horizontally to reach the acromion and spine of the scapula. Its thoracic fibres converged to the deltoid tubercle of the scapula (see Figure 1).
Figure 1: Anatomy of the upper trapezius
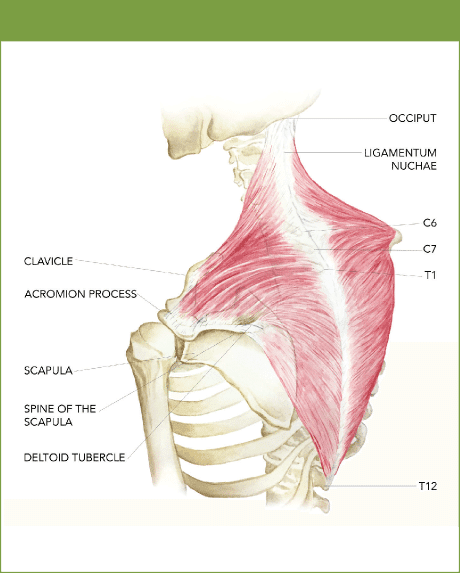
Note the thicker C7 and T1 fibres
The fascicle length of the UT fibres measured around 1cm from the occiput to C3, and from C3 to T12 the fibres were around 7-14cm. These fibres are primarily low-threshold type I fibres, suggesting that their role is not to produce power but instead act as a controller and stabiliser of the scapula.
The findings from the Johnson and Bogduk dissectionstudy paved the way for a different interpretation on the function of the UT in scapula movement. As only the upper fibres showed a vertical orientation, this suggested they may have only a slight role in scapula elevation. These fibres are
relatively small compared to the lower fibres; volumetric studies have demonstrated that the fibres from C7, T1, and the lower half of ligamentum nuchae are the largest.
Johnson and Bodguk also found that the UT muscle has an angle and orientation, which are too small to be a significant elevator of the scapula when the arm is down by the side. They act primarily as an upward rotator of the scapula when co-ordinated with the lower and middle trapezius fibres.
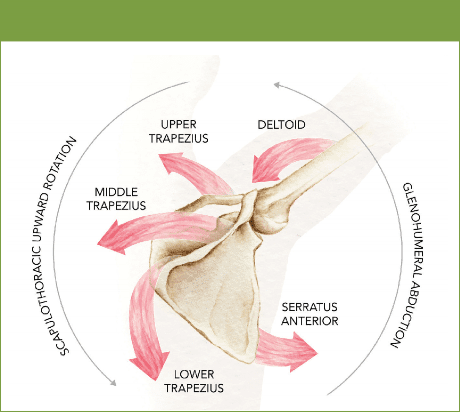
They also work in a force couple along with serratus anterior to create upward rotation. Without the contribution from the lower trapezius and serratus anterior, the UT cannot create upward rotation in isolation. It needs to work in concert with the other upward rotators.
The mechanism of this force couple is via the action of the serratus anterior, which pulls the scapula into protraction. The lower trapezius contracts isometrically to fixate the middle medial border of the scapula so that the serratus anterior can then upwardly rotate the scapula.
UT then contributes towards upward rotation as the scapula has already begun upward rotation. The UT also elevates the scapula at the top of the shoulder flexion/abduction movement (see Figure 2).
Figure 2: Force couple of UT with middle/lower trapezius and serratus Anterior
Furthermore, the majority of the UT fibres attach onto the distal third of the clavicle, and due to their horizontal arrangement, they also rotate the clavicle medially – this rotation compresses and stabilises the sternoclavicular (SC) joint.
This SC joint compression allows load to be transferred away from the cervical spine and instead is directed towards the sternum and axial skeleton.
Johnson et al argue that the increased EMG activity of the UT does not occur to elevate the scapula but instead exists to draw the clavicle medially and upward at the same time to compress the SC joint(1). Therefore, the UT creates elevation by exerting an upward moment on the clavicle and increases the
compression loads at the sternoclavicular joint. This means that the cervical spine is not taking the load of the UT during shoulder elevation but the SC joint is.
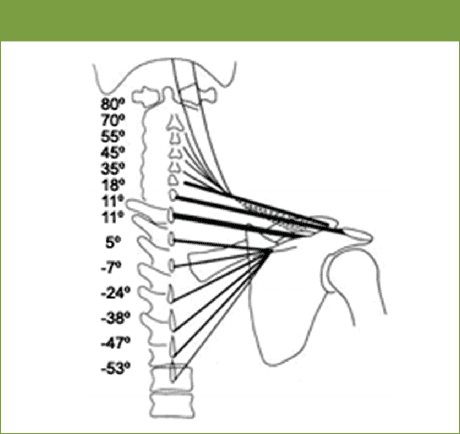
The diagram below shows the angle of orientation of the fascicles, based on the work by Johnston and Boduk(1). A radiograph shows the direction of fibres. In this image the size and cross sectional area of the fibres are also shown based on the thickness of the lines. It can be seen that the fascicles of the lower half
of the UT are much larger than the upper fibres. The largest fibres are the transverse C6 and C7 fascicles.
In summary, the UT works synergistically with the other trapezius muscles (middle and lower) to produce a force couple on the scapula; therefore the UT has both a functional role in movement and stabilisation of the scapula. To highlight the individual and synergistic role of the trapezius muscle, the individual heads work in the following ways;
Figure 3: Orientation of fascicles(1)
- UT draws the clavicle backwards, medially and upwards at the sternoclavicular joint. It helps to control the neutral positionof the scapula. It has some potential to produce movement to the cervical spine and contributes to the stability of the cervical spine.
- Middle trapezius produces scapula retractionand upward rotation, as well as drawing the clavicle and scapula backwards and medially together with UT allowing scapula upward rotation. It controls or resists scapula protraction, and downward rotation.
- Lower trapezius produces scapula upward rotation, external rotation, posterior tilt and depression. It controls or resists scapula elevation, abduction and downward rotation, as well as controlling the neutral position of the scapula.
Finally, the UT working with other cervical muscles can also laterally flex the cervical spine to the same side, rotate the cervical spine contralaterally and extend the cervical spine.
Dysfunction Of The Upper Trapezius
The UT has an important role to play in both scapula position and stability. This in turn will influence the gleno-humeral joint in positions of shoulder elevation, since scapula mobility has been linked with shoulder range of movement(2,3). During arm elevation, the scapula moves toward internal or external rotation, upward rotation, and posterior tilt. These actions are influenced by the upper/middle/lower trapezius and the serratus anterior as a force couple (mentioned above)(4). Lack of control of these muscles will break down the optimal scapula position and stabilisation/orientation of the shoulder joint. This scapula imbalance has been linked to shoulder pain(5). It must not be forgotten that other factors such as thoracic spine posture, capsule tightness in the shoulder and tightness in pectoralis major/ minor and latissimus dorsi may also influence scapula position(6,7).
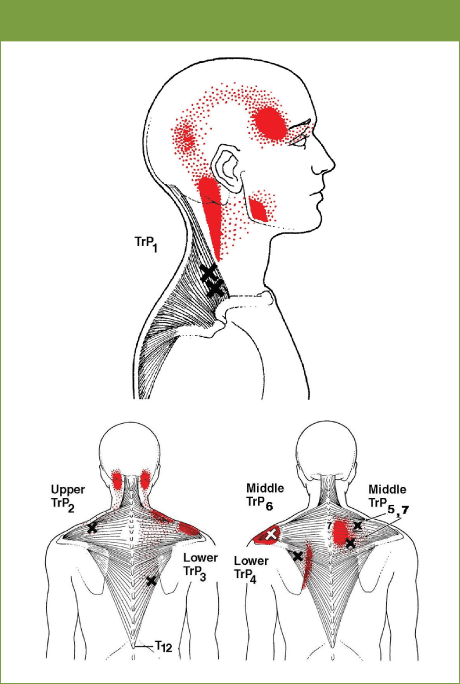
Figure 4: Classic UT trigger points (from Travel and Simons(21))
Turgot et al (2016) studied the isometric strength of the three heads of the trapezius and linked it to electromagnetic assessment of scapula mechanics(8). They found that shoulders with stronger UT muscles showed greater upward scapular rotation at 30°, 60°, 90°, and 120° of elevation in the frontal plane. Shoulders with stronger middle trapezius had greater scapular upward rotation at 90° of elevation in the frontal plane. Shoulders with stronger lower trapezius showed greater scapular posterior tilt at 90° of elevation in the sagittal plane.
Numerous studies have identified an imbalance in activation between the UT and lower trapezius in patients with painful shoulders. Specifically, the imbalance identifies overactivity of the UT and underactivity in the lower trapezius(9-13). One study found that using a novel taping technique to inhibit the UT, reduced activation patterns of the UT in patients with shoulder pain(14). This aspect will be explained in detail later in the article.
Peat and Grahame investigated trapezius, serratus anterior and deltoid EMG in people with and without shoulder pathology(15). They found that in those with shoulder pathology, UT showed increased activity during armelevationand lowering (between 40 to 100 degrees of arm elevation). Also, serratus anterior showed decreased activity at some humeral elevation angles (between 70 to 100 degrees) compared to healthy controls. This increase in UT activity has been found in numerous other studies on UT activationand shoulder pathology(9-13,15,16).
This finding may be associated with the increase in clavicular elevation or scapular elevation found in several clinical and kinematic studies(17).
The increased UT activation may be viewed as a common compensatory strategy used by people with shoulder pain and pathology to elevate their arm. However, the subsequent increase in clavicle elevation at the SC joint that may be produced by increased UT activity will result in scapular anterior tilt. This offsets the scapular posterior tilt produced at the AC joint by the lower trapezius, reducing the overall posterior tilt of the scapula on the thorax, which may be viewed as a potential mechanism to either cause or aggravate impingement symptoms.
Other authors have suggested that excess UT activity may attempt to compensate for a weak serratus anterior, and is believed to contribute to impingement through abnormal rotation
of the scapula(13). Evidence of increased UT activation combined with reduced SA activation (as well as evidence of increased superior translation of the scapula) has been demonstrated in persons with shoulder pain(13,15,18). Imbalances of force production of the serratus anterior and UT can result in a scapula elevation motion (or early shoulder shrugging). This may cause excess superior translation of the scapula, with less efficient upward rotation and reduced posterior tilting. Clinical consequences of these alterations can include subacromial impingement, subacromial bursitis, and rotator cuff or biceps tendinitis, which can progress to rotator cuff tears. There may also be altered acromioclavicular joint forces and possible predisposition to degenerative changes(19).
In a study by Leong et al (2016) (20) it was shown that athletes with rotator cuff tendinopathy exhibited higher UT shear modulus during active arm holding than the asymptomatic athletes(20) (higher shear modulus suggests an increase in active and/or passive muscle tension measured on a specialised ultrasound). UT shear modulus was also higher in athletes with rotator cuff tendinopathy than in the asymptomatic athletes during the resting arm position at 0°of shoulder abduction.
The findings from such a study cannot however be used to determine whether the increased tension in UT is a result of rotator cuff tendinopathy or if it is a cause of the problem. It is clinically appreciated that athletes with painful rotator cuff may have a scapula at rest that appears downwardly rotated and anterior tilted, and often this is attributed to an overactive pectoralis minor. This position would place extra ‘stretch’ on the UT thus creating a situation whereby the UT had to counterbalance the drag effect of the scapula position.
Upper Trapezius Myofascial Trigger Points
Figure 5: UT shrug exercise (note the wide hand placement)
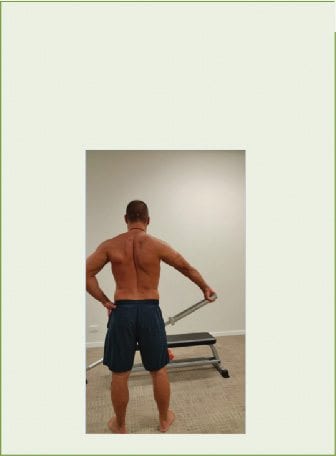
1. Wide Grip Shrug
In a study performed in Brazil, researchers attempted to correlate the anatomy of the trapezius and the accessory nerve entry points into the muscle with clinical locations of myofascial trigger points(21,22). What they found was that of the classic seven clinical points of myofascial trigger points, four correlated well to the actual anatomy of the accessory nerve and the trapezius muscle. These seven points with their characteristic referral patterns are shown in Figure 4.
Upper Trapezius, Neck Pain, Headaches & Nerve Pain
It was suggested in a study by Australian researchers that tightness in the UT is correlated to limited neural extensibility in the brachial plexus(23). Although it is difficult to prove causation, the suggestion is made that those with sensitised neural tissue may have reactive muscle tone in the UT. The weight of the arm at rest would provide a reasonable traction force to the brachial plexus, and the UT may react to protect the brachial plexus by increasing tone and lifting the scapula in order to reduce the traction effect on the nerves.
Figure 6: Single-arm overhead shrug start position (note angle of abduction)

2. Single-arm overhead shrug
What is also interesting are the morphological changes in the UT in the presence of neck pain and dysfunction.
The muscle fibre type changes from type I to type II, with fatty infiltration and higher percentage of grossly hypertrophied type I muscle mega-fibres, along with poor capillarisation(24-26). Finally, the famous ‘Janda’s Upper Crossed Syndrome’ has been implicated as a causative factor in cervicogenic headaches and patients; this condition is often present with tightness of the sternocleidomastoid, UT, levator, scalenes, suboccipitals, pectoralis minor, and pectoralis major(27-30).
Management Of Trapezius Dysfunction
*Strengthening
Figure 7: Single arm overhead shrug finish position (note external rotation of arm)

A group of Australian researchers investigated the use of a standard shoulder shrug (scapular elevation) at 0 degrees compared to a modified shrug performed with the arm elevated to 30 degrees (with the scapula in slight upward rotation). They found that the arm-elevated position elicited greater activation in the lower and upper trapezius. Therefore, traditional shrug exercises are not as effective as the 30-degree abduction position(31). Below are shown some exercises that may be used to retrain the UT in the presence of weakness and dysfunction.
Hold a barbell with the hand placed as far away as comfortably possible. This will place the arm in some abduction and the scapula in upward rotation. Slowly elevate the scapula towards the ear. Perform three sets of 20 slow repetitions with a hold. This is a great starter exercise for a patient with shoulder pathology because the arm is in relative neutral abduction.
Holding a dumbbell above the head and the body in a side sit position (this position opens up the shoulder and avoids impingement of the shoulder). Slowly elevate the scapula and rotate the dumbbell from internal to external rotation.
Perform three sets of 20 reps.
Hold two dumbbells overhead with the arm fully elevated (you need good shoulders for this). This is the same process as exercise 2 above but the exercise is performed bilaterally, and with more abduction of the shoulder.
3. Monkey Shrug
Figure 8: Monkey shrug (start position)
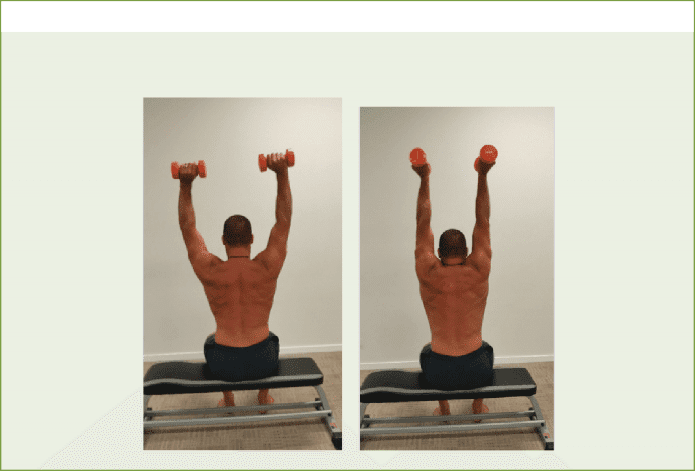
Figure 9: Monkey shrug (finish position)
*Loosening
Figure 10: Upper trapezius stretch

Figure 11: Upper trapezius trigger point (position for TrP 2 and 6)
Figure 12: Upper trapezius trigger point (position for TrP 1)
1. Upper trapezius stretch
The action of the UT is to upwardly rotate and retract the scapula; its role in elevation is questionable. The effect on the cervical spine is to laterally flex towards the same side, rotate away and finally to extend the cervical spine. Therefore, the best stretch position is one that encourages a combination of:
2. Upper trapezius trigger points
- Scapula downward rotation, protraction, depression
- Cervical contralateral flexion, flexion and ipsilateral rotation.
Above is an example of stretch to target the UT in a stretch and also ball placement for trigger point releases.
Hold the arm behind the back. This will create downward rotation of the scapula. Protract the scapula and depress the scapula actively. Pull the head to the opposite side and look over the same shoulder. Hold for ten seconds and repeat five times.
Place a ball (tennis, spikey, trigger ball) into any of the seven mentioned trigger points. Hold against the trigger for 30 seconds, move off and find another spot.
Conclusion
The UT is an important muscle of the scapula, which has a major role in scapulohumeral rhythm. Its key roles are scapula upward rotation, elevation and retraction. Its role as a scapula elevator is not as important. It is a muscle that may become either tight and hypertonic as a compensatory mechanism for other scapula imbalances, or it may become weak as it is dragged into a stretch position by poor scapula posture. Exercises have been presented that are designed to either strengthen the muscle or to release tightness and hypertonicity.
References
1. Clin Biomech (Bristol, Avon). ;9(1): 1994. 44-50
2. Am J Sports Med, 1998, 26: 325–337
3. Journal of the American Academy of Orthopaedic Surgeons. 2003, 11, 142–15
4. Clin Orthop Relat Res, 1996, (330): 3–12
5. Orthop Clin North Am, 2000, 31: 285–293
6. J Orthop Sports Phys Ther, 2009, 39: 90–104
7. J Phys Ther Sci, 2015, 27: 1739–1742
8. J. Phys. Ther. Sci. 2016. 28: 1864–1867
9. The Physician and Sportsmedicine, 2003. 31(7), 25–32
10. Mottram, S. L. (1997). Dynamic stability of the scapula. Manual Therapy, 2,123–131
11. Journal of Orthopaedic and Sports Physical Therapy, 1999. 29, 31–38
12. Am. J. Sports Med. 2003. 31; 542-549
13. Physical Therapy Mar. 2000. 80(3):276-291
14. Phys Ther Sport 10 (2), 45-50. 2009
15. Am J Phys Med 1977;56(5):223–40
16. J Electromyogr Kinesiol 2005;15(6): 576–86
17. Phys Ther 2006;86(8): 1075–90
18. J Orthop Sports Phys Ther. 1999. 29: 574–586, 1999
19. American Journal of Sports Med. 2004. 32(2); 484-493
20. Leong et al (2016) Increased Upper Trapezius Muscle Stiffness in Overhead Athletes with Rotator Cuff Tendinopathy. PLoSONE 11(5)
21. Travel and Simons (1999) Myofascial pain and dysfunction. Volume 1. Upper half of the body. Second edition. Williams and Wilkins. Baltimore.
22. Akamatsu et al (2015) Biomed Research International 2015.
23. Australian Journal of Physiotherapy. 1994. 40(2); 99-103
24. Manual Therapy. 2008. 13: 258–265
25. Spine. 2004. Vol 29(13) 1 July:1436-1440
26. Journal of Electromyography and Kinesiology. 2008. 18:255–261
27. Cephalalgia, 1994. 14(4): p. 273-9
28. Cephalalgia, 1999. 19(3): p. 179-85
29. Man Ther, 2006. 11(2): p. 118-29
30. The International Journal of Sports Physical Therapy. 2011. 6(3); 254-266
31. Clinical Biomechanics. 2014. 29(2): 201-205
Post Disclaimers
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Upper Trapezius: The Key To Optimal Function Of The Shoulder" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933





Comments are closed.